
Predicting Hospital Readmission Following Acute Kidney Injury
- Cheng-Yi Li
- Emma Meihofer
- Nicolas Jos
- Ruihan Yuan
- Zixi Xiao
- Maya Sharma
- Joseph L. Greenstein
- Casey Overby Taylor
- Heather Thiessen Philbrook
- Jack Bitzel
- Chirag Parikh
Abstract:
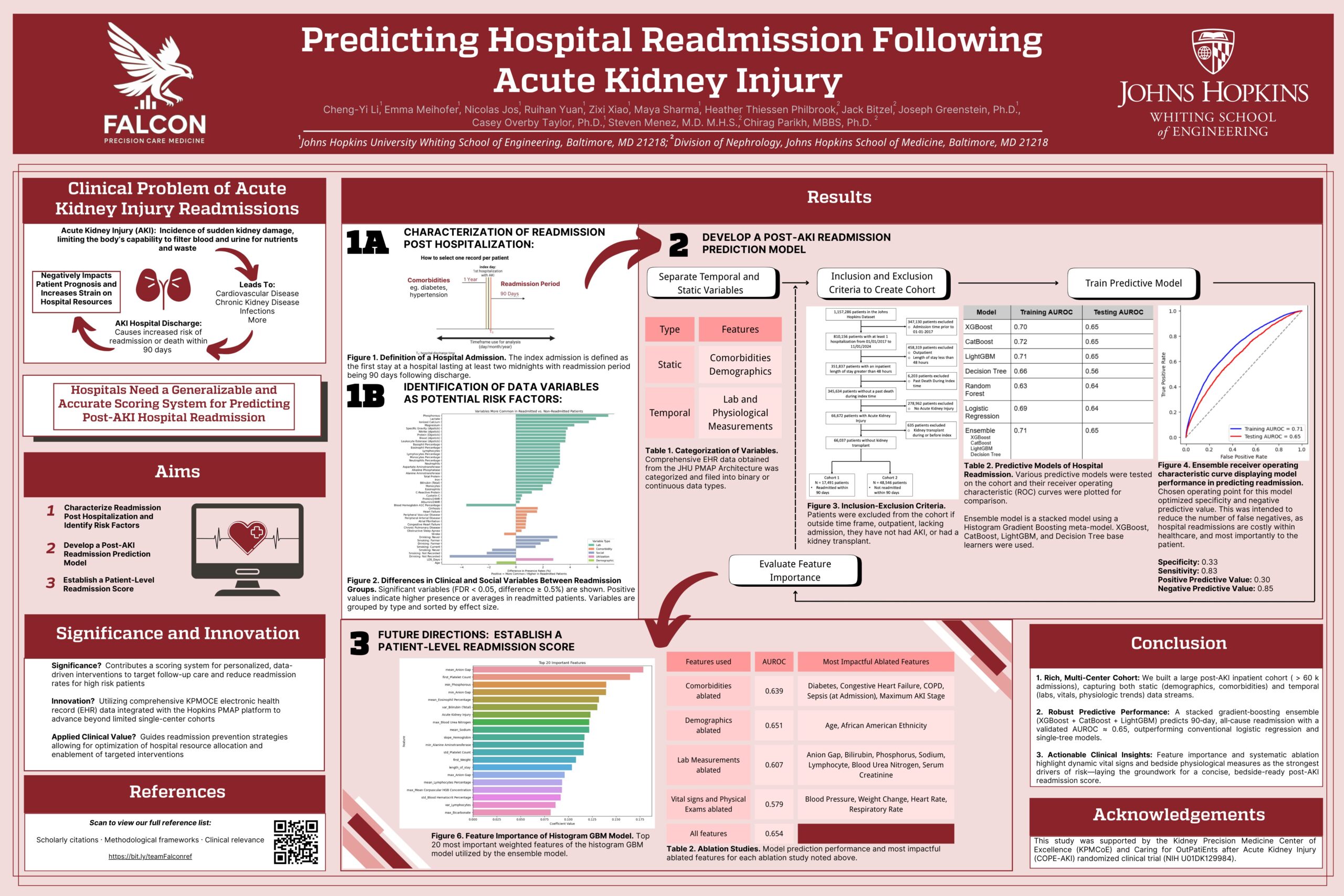
Acute Kidney Injury (AKI) is a sudden loss of renal filtration capacity that leads to toxin and fluid accumulation. Patients who survive AKI-related hospitalizations are frequently readmitted, contributing to poor outcomes and healthcare strain. However, existing readmission risk tools are often based on small, single-center cohorts and lack generalizability.
To address this, we linked the Johns Hopkins Precision Medicine Analytics Platform with Kaiser Permanente Mid-Atlantic EHR data to construct a large, multi-center post-AKI cohort of over 60,000 admissions, integrating demographics, comorbidities, lab trends, vital signs, and other physiologic data. We trained a stacked gradient boosting ensemble that achieved an AUROC of ~0.65 for predicting 90-day all-cause readmission—outperforming logistic regression and single-model baselines.
Systematic feature analysis identified dynamic vital signs and bedside physiologic measurements as key predictors, supporting the development of a concise, clinically actionable risk score to identify high-risk patients and guide targeted post-discharge interventions.
{kind=link}